All about ED...
 Elbow
dysplasia (ED) is a general term used to identify inherited
polygenic diseases of the elbow in dogs. Affected
animals may exhibit intermittent lameness or an abnormal gait which is aggravated by exercise
or when the dog first moves following prolonged rest. Watch out for sudden or gradual front leg
lameness, morning stiffness or stiffness after a period of rest. In this technical article, vet
Peter van Dongen goes through the anatomy of ED. Elbow
dysplasia (ED) is a general term used to identify inherited
polygenic diseases of the elbow in dogs. Affected
animals may exhibit intermittent lameness or an abnormal gait which is aggravated by exercise
or when the dog first moves following prolonged rest. Watch out for sudden or gradual front leg
lameness, morning stiffness or stiffness after a period of rest. In this technical article, vet
Peter van Dongen goes through the anatomy of ED.
Elbow Dysplasia (ED) is an abnormal development of the elbow joint and includes several primary
specific abnormalities affecting different sites in the joint. These abnormalities involve the
cartilage, which makes up the surface of the joint itself, or the other structures of the
joint, such as the bones themselves, the synovial membrane and the ligaments and tendons
surrounding the joint. The primary abnormalities cause secondary changes such as osteo-arthritis
(arthrosis, degenerative joint disease (DJD)) due to excessive wear and tear of the joint. Most
primary lesions occur in the young growing animal and are often present in both left and right
elbow joint.
 The Elbow Joint The Elbow Joint
The
elbow joint works like a hinge and allows movement mainly in one plane only. It is made up
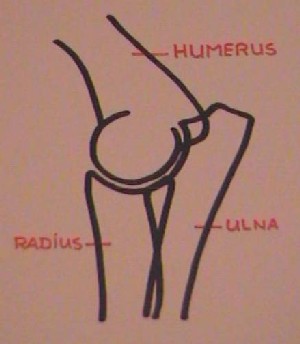
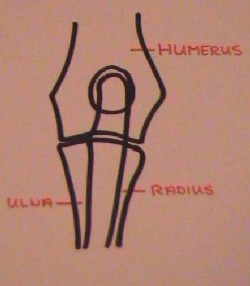
of three bones, which normally fit together perfectly (See photo and line drawings).
The single bone of
the upper foreleg is called the humerus, the two bones of the lower foreleg are called the
radius and the ulna. The ulna is the longer one, which makes up the point of the elbow,
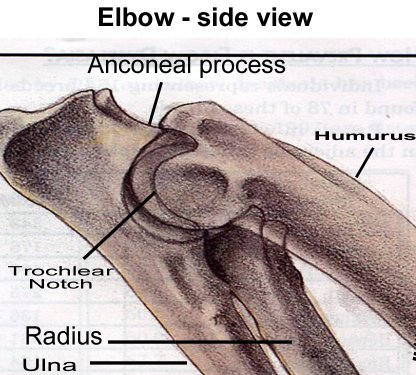
called the olecranon. The distal (furthest away from the body) part of the humerus is
called the condyle, which has a medial (towards to inside of the body) and lateral (towards
the outside) part. The proximal (closest to the body) part of the ulna has a medial and
lateral coronoid process and an anconeal process, in between which the trochlear notch
articulates with the humerus. The proximal part of the radius is called the radial head.
The ends of the bones are all covered by hyaline cartilage (joint cartilage) which is
normally very smooth. The joint is surrounded by a synovial sac, called the joint capsule,
which contains the synovial fluid (joint fluid) to help lubricate the joint. The bones are
held together by means of ligaments (collateral ligaments), one on either side of the
joint. In addition several tendons cross the joint on either side.
If there is any
change to the anatomical build of any part of the above, the joint will not fit together
properly, leading to damage to one or more of the structures involved and an excessive wear
and tear of the joint. The elbow joint is particularly prone to these changes as it is the
major point of movement of the foreleg. The other joints of the foreleg, shoulder and
carpus (wrist) do not move as much during the normal locomotion of the dog.
Causes of Elbow Dysplasia
Elbow dysplasia is a multi-factorial disease, which means that there are several factors
which can influence the occurrence of the condition. The genetic make-up of the dog is by
far the most important factor. Furthermore there are many factors which influence the
chance of developing ED or the severity of the problem, such as nutrition, hormonal status,
growth rate and exercise level. The latter factors can not cause or prevent the disease on
their own and they can not influence the way that the disease is passed on to a dog’s
offspring.
 Genetics Genetics
As
mentioned above, the most important factor in the development of ED is the genetic make-up of a
dog. Unfortunately the disease is controlled by a number of genes (it is ‘polygenic’) and this
makes for a complicated inheritance. It also means that certain breeds of dog are more prone to
the development of ED than others, as many dogs within one particular breed have a large number
of genes in common. In general, these are the medium-to-large and giant breeds.
The breeds which are prone
to any particular primary condition are mentioned below. Males are affected more often than
females, possibly due to their faster rate of growth or heavier build. One of the problems in
deciding which dogs to breed from is the fact that many dogs which are affected genetically, or
even anatomically, are not necessarily affected clinically. They may not show any clinical
symptoms such as lameness. These dogs are called sub-clinical dogs. They can only be detected
radiographically at the moment. In the future perhaps there will be DNA tests available to
assess the genetic make up of a dog for a particular trait.
Primary
Lesions
-
Osteo-Chondritis Dissecans (OCD)
This condition affects the distal aspect of the medial part of the humeral condyle, where
it articulates with the ulna. It causes thickening of part of the articular (joint)
cartilage, which is then prone to fibrillation, fissuring and separation. If a flap
forms, this can become detached and ‘float’ inside the joint (‘joint mouse’) which leads
to intra-articular inflammation. Sometimes the thickened cartilage can be seen as a
‘defect’ in the bone contour on radiographs (x-ray films) on some views, but usually this
condition is not actually seen itself on radiographs, only the secondary changes which
result from the condition. When a loose flap is formed this can sometimes become
mineralised, in which case it can be seen.
- Fragmented (or
un-united) Coronoid Process (FCP)
This condition affects the proximal aspect of the ulna on the medial side. It leads
to a fragmentation and/or fracturing of the coronoid process, where the ulna articulates
with the humerus. This in turn leads to joint inflammation and secondary changes as
above. The primary lesion is very rarely seen on radiographs, even on good quality
radiographs. This is the most common primary condition causing elbow dysplasia.
- Un-united
Anconeal Process (UAP)
This condition affects the proximal aspect of the ulna at the top of the trochlear
notch. The anconeal process sometimes has a separate centre of ossification, which means
it develops separately as part of the boney ulna from cartilage and joins the shaft of
the ulna later. Between the anconeal process and the shaft of the ulna lies a growth
plate (physis), made up of cartilage, which contributes in part to the growth in length
of the ulna. When the anconeal process does not join the rest of the ulna, we call this a
UAP. In about 40% of cases it affects both left and right elbow.
- Un-united
Medial Humeral Epicondyle
This, much more rare, condition affects a part of the distal humerus, just proximal
to the medial aspect of the humeral condyle. Again, this part of the bone has a separate
centre of ossification and sometimes fails to joint the rest of the humerus. It generally
causes a milder form of lameness than the other primary lesions.
- Short Radius
Syndrome
This is a condition where the radius has not grown at the same rate as the ulna,
leading to an incongruency of the elbow joint, called a subluxation. It is usually caused
by a premature closure of one of the growth plates (physes) of the radius. It is quite
rare, and often thought to be the result of trauma to the growth plate.
- Short Ulna
Syndrome:
This is a condition where the ulna has not grown at the same rate as the radius due
to premature closure of the distal ulna growth plate. It leads to a similar elbow
subluxation as short radius syndrome.
- Congenital
Dislocation of the Elbow
There are two forms of this condition, where the elbow joint has not been formed
properly from birth. It leads to a malformation of the joint, again leading to joint
incongruency and subsequent arthrosis. In one form of there is lateral (outwards)
rotation of the ulna. In the second form of Congenital Dislocation of the Elbow
there is caudo-lateral (backwards and outwards) luxation of the radial head.
‘Osteochondrosis’
This term is often used inconsistently or confusingly for one or several of the
conditions above. Osteochondrosis is a developmental orthopaedic condition in which a
disturbance in the normal process of endochondral ossification results in a thickening or
retention of articular or physeal cartilage. The thickened cartilage is then prone to
fibrillation, fissuring and separation. If a cartilage flap develops in articular cartilage,
intra-articular inflammation and degenerative joint disease may result and the condition is
then most appropriately described as osteochondritis dissecans (OCD).
Endochondral ossification
is one of the two processes in which bones are formed. In this case bone develops on a
preformed cartilagenous matrix, either at the end of the bone or in the physis. It is the main
process behind the growth in length of the long bones in the body.
Intra-membranous
ossification is the second process in which bones are formed. In this case bone forms in bands
of connective tissue. This happens in flat bones, such as the skull bones and the pelvis, and
it is also the way in which bones grow in width. The primary conditions 1-6 are all thought to
be due to osteochondrosis.
Symptoms
The
symptoms of elbow dysplasia are dependent on the particular condition present in the patient
and the chronicity of the problem. Generally it causes lameness, although this can be very
subtle and easily missed by an owner, particularly as the problem often occurs in both legs at
the same time. In such cases it often causes a minimal stiffness rather than a true lameness.
It can also cause pain, especially on manipulation, such as extension, flexion and rotation
on the joint. The lameness is often a ‘starting lameness’, which gets better as the patient
‘warms up’ and sometimes intermittent in nature. This is similar to the type of lameness seen
in older patients with degenerative joint disease. The most reliable way to make a
diagnosis is radiography (x-raying).
 Radiography Radiography
Radiography is used to detect either the primary lesion itself or the subsequent degenerative
joint disease. Normally three different views are taken of each joint to fully assess the joint
structures, two in a lateral plane (with the x-ray beam directed sideways through the joint,
whilst extended and flexed) and one in the cranio-caudal plane (beam directed from the front of
the joint to the back of the joint). Different areas of the joint are more clearly identifiable
on each view. As already mentioned above, not always is it possible to identify the primary
condition present in the joint, but it is usually possible to detect the secondary changes.
Together with the clinical symptoms, the age of the patient and more importantly the breed, it
is often possible to come to a definite diagnosis.
Prevention
Prevention of Elbow Dysplasia is based on sensible breeding, using only dogs not affected or
only very mildly affected by the condition. To this purpose it is necessary to radiograph each
and every dog, as there are many dogs with radiographic evidence of elbow dysplasia, but
without any clinical signs. These ‘sub-clinical’ cases would be missed if they were not
radiographed. Only dogs who have no, or only very minor, radiographic evidence of elbow
dysplasia should be used for breeding. In the UK the ED scheme has been operational for the
last few years to this purpose. This scheme is run by the British Veterinary Association and
the Kennel Club together, according to guidelines by the International Elbow Working Group.
Dogs examined under the
scheme are radiographed as described above, at an age of at least one year old, and the
radiographs are then sent for examination by a select group of scrutinisers who have extensive
experience in the assessment of radiographs. A grade for each elbow of each patient is decided
upon, based on the presence or absence of primary lesions, as well as the presence or absence
of any secondary changes in the joint. The score for each elbow can be: 0 if the joint is
normal, 1 when there is mild ED, 2 if there is moderate ED or any primary lesion, and 3 if
there is severe ED. The overall grade for each individual patient is the highest of the two
scores, not the total, as in the hip scoring system. Only dogs with scores of 0 or 1 should be
used for breeding purposes. The results of any dog radiographed under the ED scheme are kept on
record by the Kennel Club. The effect of this system will only really be seen after several
generations of selective breeding in the affected breeds.
Treatment
Treatment
of ED depends on many factors, such as the nature and severity of the primary problem.
Conservative treatment, such as weight control and exercise control, are important in each and
every case. In a number of cases, drugs, used to reduce pain or inflammation, are needed.
Furthermore, in some cases surgical intervention is necessary. In some cases nutritional
supplements are useful to reduce the possible future build up of arthritic changes. Other forms
of treatment include physiotherapy, homeopathy and acupuncture. Nearly all dogs can be managed
successfully, if the symptoms are recognised and the dog is diagnosed early on in the disease
process.
Breeds most prone to ED
OCD: Labrador Retriever, the Golden Retriever and the Rottweiler.
Symptoms usually develop between 4-5 months of age.
FCP: Labrador Retriever, the Golden Retriever, the Rottweiler, the
German Shepherd Dog and The Bernese Mountain Dog. Other breeds affected are the St.
Bernards, Chows, Rhodesian Ridgebacks and Newfoundlands. Symptoms usually develop between
4-5 months of age. Sometimes FCP and OCD occur in the same joint at the same time.
USP:
German Shepherd Dog and the Bassett Hound. More rarely we see it in Wolfhounds, Rottweilers,
St. Bernards and Great Danes. Symptoms usually develop between 4-5 months of age.
Un-united Medial Humeral Epicondyle:
Labrador Retrievers are prone to this condition.
Short Ulna Syndrome: Great Danes, Irish Wolfhounds and the Bassett
Hound or after trauma.
Congenital Dislocation of the Elbow - (lateral (outwards) rotation of the
ulna. This is mostly seen in Shelties, Pekingese, Cocker Spaniels, Yorkshire Terriers,
Boston Terriers, Miniature Poodles, Pugs, Chihuahuas and Miniature Pinschers. It is usually
recognised within the first three months of life.
Congenital Dislocation of the Elbow (caudo-lateral (backwards and
outwards) luxation of the radial head. This is mostly seen in Pekingese, Yorkshire
Terriers, Pomeranians, Staffordshire Terriers, Boxers, Bulldogs, Bull Mastiffs, Old English
Sheepdogs and Rough Collies. Affected animals are often 4-5 months old at presentation.
 About
the author... About
the author...
Peter van Dongen
qualified as a vet at the Utrecht Veterinary school, The Netherlands, in March
1990. He worked in a mixed practice in Louth, Lincolnshire, UK, for 3 years, before moving to
Borough Green, Kent, UK. At the same time he limited himself to small animals only. Since
December 1996 he has run his own branch practice in Allington, Maidstone, UK.
In May 1995 Peter started agility (after years of just thinking about it!) with
his Jack Russell Cross 'Basil' (a bitch!), then 5 years old. Since then they have qualified for
many finals, including 'Crufts' and 'Olympia'. Basil won the coveted Crufts 2001 title in the
individual mini agility.
Peter passed the British Agility Club Instructors' exam in October 1999 and has
since done the British Agility Club Judging Workshop.
Peter regularly writes for various agility magazines and web sites and has been
the official British Team Vet for the Agility World Championships for the last three years.
Peter and his wife Carry still live in Borough Green with their two dogs and two
cats. His little Jack Russell X, Sky, has just started agility training and will hopefully
follow in Basil’s footsteps!

Q.&A.
The term
elbow dysplasia (ED) is a general term that is used to describe a developmental degenerative
disease of the elbow joint. Understanding the symptoms and causes of ED is extremely important
if informed decisions are to be made regarding diagnosis, treatment, and prevention of ED. The
Working K-9 Vet Dr. Henry de Boer discusses this crippling disease, its causes and symptoms and
diagnosis along with its treatment and prevention.
Q. I have been hearing a lot about elbow dysplasia
recently. What exactly is elbow dysplasia? Are there symptoms I should be watching for in my
young dog?
A. There are in fact three different etiologies that can
create a diagnosis of ED. These etiologies may occur individually or in combination with each
other in any one dog. This disease has created considerable confusion and controversy not only
on the part of dog owner, but with practicing veterinarians as well as researchers who are
studying the problem. While our ability to diagnose ED has improved in recent years, there is
still a great deal to be learned about its causes, prevention, and what constitutes appropriate
treatment.
ED occurs predominantly in medium or larger breeds of
dogs. The Orthopedic Foundation for Animals (OFA) maintains statistics in their elbow registry
for many breeds. As of December 31, 1998, ED had been diagnosed by OFA in 87 breeds. Incidences
range from 0% in Border Collies up to 47.8% in Chow Chows. The average incidence of the breeds
for which at least 75 individuals have been evaluated is 11.11%. Male dogs are more likely to
have ED then females, and 20-35% of dogs with ED have it in both elbows.
Dogs with ED may or may not be lame, therefore, using
lameness to determine its presence or the breed worthiness of an animal is foolhardy. Dogs with
clinical ED typically develop foreleg lameness between the ages of 5-12 months of age, however,
in some cases the lameness may not be apparent until as late as 5-7 years of age. The lameness
may be variable and periodic. Some dogs may demonstrate soreness after rest, improve slightly
with activity, but then worsen with increased activity. There may be intervals with no lameness
at all. Jumping and sharp fast turns usually exaggerate the lameness. Pain can be elicited by
overextending the elbow, and there may be a slight to moderate swelling noticeable when
carefully feeling the elbow joint. If both legs are meaningfully affected the lameness may be
more difficult to detect. Careful observation would show slight rotation of the top of the paws
outwardly, as well as a stiff or stilted movement of the forelegs. There may be a reluctance on
the dogs part to land hard on the front legs (e.g. trotting, loping or landing jumps).
 For the sake of
simplicity the three etiologies resulting in ED will be discussed individually, but it is
important to note that there can be considerable overlapping in their presence, their cause and
effect. The magnitude of the overlapping has probably not been fully realised at this time. For the sake of
simplicity the three etiologies resulting in ED will be discussed individually, but it is
important to note that there can be considerable overlapping in their presence, their cause and
effect. The magnitude of the overlapping has probably not been fully realised at this time.
The anconeal process is a small pyramid shaped
piece of bone on the upper end of the ulna. In a young dog, it is a piece of cartilage that
gradually turns to bone and unites with the rest of the ulna at approximately 4 ½ - 5 months of
age. If that union fails to take place we have an ununited anconeal process (UAP). The presence
of UAP leads to degenerative joint disease as a result of a decrease in stability within the
joint, and an increase in inflammation caused by the chip of bone being free within the joint.
Osteochondritis dessicans (OCD) can occur in many joints,
but when it occurs in an elbow it most commonly is on the lower, inner aspect of the humurus
(medial humural condyle). In essence OCD is a vertical fracture in the articular cartilage of
the humurus, which can lead to a flap of cartilage within the joint. This flap leads to
degeneration within the joint as a result of an inflammatory process.
 The
coronoid process is a small piece of bone on the ulna, which articulates with the humurus.
Similar to the anconeal process it starts as cartilage, and gradually turns to bone as it
unites with the rest of the ulna. Failure of that fusion to occur or chipping of the area after
fusion has occurred, creates a fragmented coronoid process (FCP). Subsequent to FCP
degenerative joint disease develops for the same reason as with UAP. The
coronoid process is a small piece of bone on the ulna, which articulates with the humurus.
Similar to the anconeal process it starts as cartilage, and gradually turns to bone as it
unites with the rest of the ulna. Failure of that fusion to occur or chipping of the area after
fusion has occurred, creates a fragmented coronoid process (FCP). Subsequent to FCP
degenerative joint disease develops for the same reason as with UAP.
Causes
The exact causes of ED have been the subject of considerable controversy. A number of
predisposing factors have been identified, and recently some new theories have gained support
as probable explanations for the development of ED. The individual etiologies of ED most likely
have multiple possible causes.
OCD has at least three possible causes.
- Heredity certainly plays a role, as we do see a
tendency for this problem to occur in family lines, as well as in those breeds that grow
rapidly.
- Trauma within the joint also is a factor, evidenced by
the fact that areas commonly affected by OCD are those that typically experience high levels
of biomechanical stress. Additionally, animals housed on hard surfaces are more likely
statistically to have a higher incidence of OCD.
- A third cause is a lack of sufficient blood supply to
the joint cartilage. The specific cause of this marginal blood supply is not currently
understood.
Understanding of the causes of FCD and UAP has
experienced a surge in recent years. In addition to the causes listed for OCD, recent research
strongly suggest that two factors are playing a major role in the development of these two
etiologies. A disparity in the growth rate between the radius and ulna, as well as an abnormal
formation of the trochleor notch in the ulna, have been implicated in the development of ED.
The elbow joint is a very complex joint that is created by the junction of three different
bones. Normally these bones fit and function together with very close tolerances. If the growth
rate of the bones is changed, or a structure does not form normally, the tolerances change,
enhancing the possibility of damage within the joint. The damage created typically results in
either FCP or UAP.
Diagnosis
The term elbow dysplasia (ED) is a general term that is used to describe a developmental
degenerative disease of the elbow joint. There are three component causes:-
- Osteochondritis dessicans (OCD)
- Ununited anconeal process (UAP)
- Fragmented coronoid process (FCP)
In general elbow dysplasia should be suspected as a
possiblity with any foreleg lameness that persists for more than several days, especially if
the dog is of a breed that may be prone to ED. Examination of the leg yields pain on palpation
when the elbow joint is over-extended. The next step in establishing a diagnosis is having high
quality radiographs taken. Multiple views of the leg should be taken, and if ED is evident,
radiographs of the other elbow are appropriate given the possibility of this problem occurring
in both elbows. UAP is easily detected with radiographs, and in most cases, a diagnosis of OCD
can be made with radiographs as well. FCP can be diagnosed in most cases with radiographs, but
can be a challenge in yet other cases. The problem is that the coronoid process is a relatively
small piece of bone that in the majority of standard radiographic views cannot be visualized by
itself, but rather is superimposed on the other bony structures within the elbow. Given that
superimpositon, if the lesion is small, it may be difficult if not impossible to see. In many
of the cases in which the coronoid process cannot be visualized there will be bony changes in
other areas of the joint that will strongly suggest FCP. If the information from the
radiographs is equivocal, a CT scan can typically help significantly in establishing a firm
diagnosis. While CT scans are not readily available in all local areas, they are generally
available at least regionally, and are a very valuable diagnostic tool for this problem.
The approach to diagnosing ED is consistent, however the
approach to treating the problem is variable. Developing a treatment protocol for ED depends
not only on the etiology, but also on the symptoms that the dog is demonstrating, as well as
the duration of the problem.
Treatment
UAP traditionally has been a problem that has been treated surgically. In the past, one of two
surgical options have been used. In the first, the fragment of bone within the joint has been
removed, and in the second, the fragment has been reattached using a lag screw. In general,
dogs undergoing either of these surgeries have improved to an extent clinically, but in many
cased, degenerative joint disease continued to develop and there is typically some loss of
stability within the joint and/or some sporadic lameness. For working dogs these results have
been less than impressive. Recently a new surgical approach to the problem has been developed,
in accordance with the theory that a disparity in growth rates between the radius and ulna is
to blame for the development of the UAP. In this surgery a small slice of bone is removed from
the ulna, which prevents the disparity in growth rates from creating tension within the joint.
This decrease in tension allows the anconeal process to unite, followed by healing of the ulna.
Early reports from those surgeons using this technique have been extremely encouraging. In a
high percentage of these cases the anconeal process is uniting, there is minimal degenerative
change and no instability within the joint. This procedure, in my opinion, is very promising
for our working dogs. It is important to note that for this procedure to be beneficial the
problem must be diagnosed as soon as possible. The anconeal process, in most dogs unites
normally at approximately five months of age. Radiographic screening can be done at five to six
months of age, and, in most cases no sedation or anesthetic would be necessary for the
radiographic view required.
Treatment of FCP or OCD can be medical or
surgical/medical. I typically recommend that most dogs with FCP or OCD be treated medically at
first, and if the results are not satisfactory, surgery should be considered. Medical
management would include a moderate exercise restriction as well as a dietary change if
warranted. The dietary alteration would be to achieve weight reduction if required and to alter
food intake so as to keep growth rate at a relative minimum. The use of chondroprotective
agents such as Cosequin, Glycoflex or similar products is appropriate, as well as the use of
non steroidal anti-inflammatory medications. If after five to eight weeks, the results of
medical management is not satisfactory, surgery can be performed. The surgical technique for
both FCP and OCD essentially results in removal of the adversely affected area. Surgery should
be followed by the ongoing administration of chondroprotective agents and anti-inflammatory
medication if required.
The results of surgical/medical management are generally
satisfactory, with some animals experiencing substantial relief but some others showing only
moderate improvement. The prognosis for a working dog that has had surgical repair for FCP or
OCD being able to work pain and lameness free is fair, and there is a moderate probability of
early degenerative joint disease (arthritis).
Prevention
Prevention of elbow dysplasia can indeed be a frustrating endeavor. While some of the causes
are known, the level of understanding as to their relative importance, and how they relate to
each other is still being examined. The primary factors we need to be conscious of are:
genetics, nutrition, and trauma.
ED clearly has a genetic basis, however, it is not highly
predictable as to which dogs will be affected by its presence. This lack of predictability
eliminates our ability to confidently select breeding stock or puppies it they are from a breed
that is predisposed to ED. In spite of this low level of predictability, every effort should be
made to eliminate this problem. The Orthopedic Foundation for Animals (OFA) does have an elbow
registry that will certify elbows at two years of age. They will give preliminary evaluations
at any age, and given the surgery available for UAP, screening at five to seven months of age
would certainly be prudent. Any dog with radiographic evidence of ED, whether or not they are
lame, should probably be eliminated from breeding. It is important to note, however, that dogs
with low level changes in an elbow (Grade 1 ED) may never develop any lameness whatsoever.
Working these dogs is appropriate as long as the handler is mindful of the possibility of a
future lameness. Clearly, if these dogs are being worked, weight should be kept at an
appropriate level, and those exercises requiring hard landing on the forelegs should be
minimized. Additionally, dogs with very low level changes on a preliminary evaluation should be
re-evaluated in six to twelve months. Changes in an elbow that appear significant at a young
age may be insignificant at an older age a long as there has been no progression in the
changes. These dogs could potentially be clear of ED at a mature age.
Nutrition has also been shown to play a role in the
development of ED. The specific factors that have been shown to be of particular consequence
are the feeding of high energy foods, especially if fed in excessive volumes, and the level of
calcium in the diet.
Rapid growth has been shown to increase the risk of ED.
Every effort should be made in those breeds predisposed to ED to keep their growth rate as low
as possible by keeping food volumes as well as the energy content low. A higher energy content
of a diet increases the likelihood of a dogs consumption surpassing its requirements. Since fat
is a substantial component of energy density, fat content of a chosen diet for young dogs
should generally be below 17%. Total energy density should be kept below 4.0 kcal/g. This
information should be available from the manufacturer of the food.
For many years it was felt that the ratio of calcium to
phosphorus in a diet was more important than the absolute volumes. This has been shown to be
inaccurate, and current recommendations are that calcium levels should be approximately .9 –
1.5% on a dry matter basis.
In recent years there has been a tremendous surge in
nutritional supplements for dogs. Inasmuch as ED is concerned (as well as other skeletal
developmental abnormalities) supplementation has the potential to create far more problems than
it can prevent. Beware!
Trauma to growing and developing joints can also play a
role in ED. Quantitating the effect of trauma is difficult at best, but common sense would
suggest that while we want to keep young dogs in good physical condition, we should minimize
those activities that would create high impact on developing joints.
Clearly, ED is a complex entity which much has been
learned about in recent year, but much more needs to be done if we are to decrease its
frequency, as well as its effect on our dogs. Hopefully, the increased awareness of ED on the
part of dog owners, as well as continued veterinary research will lead to a significant
decreases in the frequency and severity of this nagging problem.
OFA (Orthopedic Foundation for Animals) is looking for a
former competitor (any breed, actually) who may have been videoed running an agility course
healthy, who subsequently developed ED. They are putting together a film about ED, and the
purpose would be to demonstrate the impact of the disease on competition. A dog living near St
Louis would be ideal, as they might want to include a snippet on the current condition of the
dog.
If your current or former partner fits this and you would
like to participate, contact Ann Green on algreen@panix.com.
 Dr.
Henry De Boer is the Working K-9 Vet. Following
his 1973 graduation from Cornell University, he established Pioneer Valley Veterinary Hospital,
based in western Massachusetts. Dr.
Henry De Boer is the Working K-9 Vet. Following
his 1973 graduation from Cornell University, he established Pioneer Valley Veterinary Hospital,
based in western Massachusetts.
His involvement with working dogs dates to the mid-1960’s
when he began training and handling hunting dogs. In 1984 he became involved with the sport of
Schutzhund and has gradually risen to the level of national competitor.
Through the years. De Boer has worked both in a training
and veterinary capacity with a wide variety of working dogs. His knowledge and enthusiasm for
working dogs led to the establishment of Working K-9 Veterinary Consultation Services. This
service provides veterinary consultations for working canines and is available by phone, fax,
or email.
Tel/fax: (+01) 802-254 1015. Or visit http://www.workingk-9vet.com
Picture credits: Orthopedic Foundation for
Animals and Gheorghe M. Constantinescu DVM
Comment:
Here's a totally anecdotal personal experience. (I'm not a veterinarian.)
When I adopted my BC at five months of age, I had his
hips x-rayed without anesthesia. His hips deemed fine at that time.
He became acutely lame in the rear at around two years of
age, and I had him x-rayed again under anesthesia. He was mildly dysplastic. I went into a
tailspin, because I'd already had some pretty nifty wins with him in Novice obedience and was
afraid he'd never be able to jump in the Advanced classes. At that time, I didn't know a single
dog who'd had hip surgery that I considered sound enough to jump. That has changed since then,
and I know lots of dogs who could do obedience jumping after surgery.
Then I got lucky.
A good friend sent me literature on CHD that (I think)
had been put out by the national Labrador club on CHD based on findings by OFA. One thing it
said was that many mildly dysplastic dogs experience acute lameness at around two years of age.
Even with no treatment at all, many of them adjust to it and show no lameness for many years
afterward.
When I told my vet that I was dubious about hip surgery,
he said that he'd recommended one hip surgery in 15 years of practice. He said that proper
exercise to maintain rear-end muscle tone and joint supplements kept all but the most extreme
cases pain-free well past their middle years with no restrictions on their performance
activities. (This was before agility came on the scene, co I can't tell you he'd say the same
today.)
Jack went on to earn his CDX and run in sheepdog trials
until he was nine years old. He's 11 now and still exhibits no lameness in his retirement. He
was diagnosed with moderate dysplaysia in both hips at two.
So here's my advice for what it's worth:-
Don't panic.
- Don't opt for surgery without an independent second
opinion. Keep in mind that surgeons will always suggest surgery, because that's what they do.
- Don't panic.
- Be dubious about surgery when your pup may just be in
an acute phase.
- Don't panic.
- Spay or neuter your dog to help clean up the gene
pool.
- Don't panic.
IOW, don't panic. This may not be the end of the world.
Margie English (USA)
My two cents in about running agility
with dogs who have HD and/or bad elbows...
For those that choose to run a dog with no
obvious clinical signs, so be it...
I, on the other hand, x-ray my GSDs from stem to stern
every couple of years, and if they ever showed the slightest dysplasia, they're done. I
agree muscle mass certainly helps cushion those hips, dogs may never limp or come up lame and
live to a ripe old age with HD, but I don't understand WHY anyone would want to continue
running a dog despite this?
I imagine it can be very heartbreaking to have competed
with a dog and gotten him just where you are happy only to find out they have HD or bad elbows.
Unfortunately, that can be life. I just would never want to put my dog at further risk, and I
truly believe that's what can happen by continuing. I don't see many dogs competing that have
obvious signs of problems, but there are a few, and I gotta say, it's heartbreaking to see them
doing their all for their handlers/owners despite their obvious problems.
Agility is a sport that can be physically challenging on
everyone including the dogs. It just boggles my mind that anyone would be proud of the fact
that their dog can still compete with HD or bad elbows - or would even want to! And I'm talking
downright flunking OFA ratings.. Our dogs (or at least mine anyway) and I'm sure most others,
will do anything most times, to please their owners, but would I ask my GSD to compete in
agility knowing she was dysplastic? No, I wouldn't ask it of myself let alone my dog. Just my
humble opinion.
Diane M. Stevens (USA)
 A
plea to two groups of people from Matt Tovey... A
plea to two groups of people from Matt Tovey...
Breeders: Please make dysplasia tests, and
don't breed dogs with bad scores.
Dog-owners: Please check a puppy's parents
hip-scores before buying a dog. You can save yourselves and your dog so much pain...
We took our BC Jess to the Munich veterinary clinic where
they took another very good quality x-ray and an orthopedic specialist examined her. Despite
having stopped agility and having given her medication and supplements, the specialist could
see a worsening of Jess's arthritic condition in just one month. He's advised us to stop
agility, and we will take his advice.
In preparation for German agility last year, we trained
for an obligatory obedience test. As Jess grew confident in her obedience work, she came to
enjoy that. So we plan to get her more into obedience.
It's also been very hard to see our little athlete being
crippled so, but Jess will get the best life that we can give her. We will continue to do
agility with Asterix, although trials are going to be complicated. I hate the idea of taking
Jess along, just to watch.
To read Matt & Jess' story, see
Euro-Agility.
 Go top Go top
|